


Long Covid Advocacy - Getting a Diagnosis
Written by Dr Kerry Smith Illustration by Monique Jackson (Still Ill Corona Diary)


Hi, I’m Dr Kerry Smith ( or Kerry) a GP living on the South Coast of England in Rose Cottage!
I caught Covid-19 in March 2020 whilst at work before PPE and lockdown 1.0.
6 weeks in I knew something was very wrong; I had no energy, I was dizzy on standing, I was incredibly short of breath when climbing the stairs, I had burning chest pains and my heart was racing. At some points I wondered when I went to sleep if I would wake up again the next day?
Now at 13 months after the acute infection I am left with diagnoses of Long Covid, Microvascular Angina, Positional Orthostatic Tachycardia Syndrome, Cognitive Dysfunction and in the last week Hypothyroidism. It really is the gift that keeps on giving!
During an incredibly lonely and emotional journey trying to seek validation that I was still ill and a diagnosis for my symptoms I came up against soul destroying medical gaslighting. I was really concerned that if this could happen to me as a doctor with 20+ years experience what on earth were other long haulers going through?
So I started Rose Cottage Doc, a blog on Instagram, to share how I was helping myself, to share any relevant research I discovered but mainly to advocate for other Long Covid Sufferers.
It started, due to overwhelming fatigue and brain fog, with the odd picture of compression socks or a newspaper article to now more in-depth research into all things Long Covid.
I have met some wonderful people along the way, all suffering the same, from all over the world. I really hope that my little blog has helped them in some way on their own LC journey.
I am very aware that people with Long Covid are coming up against barriers all the time. Barriers to recognition, diagnosis, validation, and care. It is for this reason that I am starting a series of posts providing “evidence” to all things LC. I am hoping that these posts will make you feel more validated about your Long Covid and can also be used to educate and inform those that are creating your barriers. To that end the posts will include evidence based medicine from journals, current research and statements from WHO and the NHS England. All references included.
There is absolutely nothing wrong in sending these references to your care provider. If you have an understanding doctor they will appreciate this. Remember they have been through the most hideous time too. Moral within the NHS is at an all time low. Demand for their time is at an all time high. Many really won’t have had time to do the extra learning required to understand LC. If we can help them a little it will, in the end, help us.
I do appreciate though that it is US that have to do the research and the advocacy for ourselves. This is incredibly difficult to navigate, frustrating, and exhausting. Sometimes even to attempt it with brain fog and fatigue is impossible. Followed then by post exertional malaise if we have taxed ourselves too much. Just do what you can when you can.
However, if your care provider is really not engaging with you and ignoring the evidence you may need to formalise a complaint. Sometimes, if you are still being treated unfairly, you may need to change provider. Do not feel guilty about doing this!
After reading from Long Covid SOS that long haulers are still being refused access to Long Covid clinics due to definitions of Covid-19 as they:
Did not have a positive PCR swab
Did not have the “correct” initial symptoms
GP refuses to diagnose them with Long Covid
So today I am stating with the simple (!) task of defining - What is a Covid-19 diagnosis?
Acute Covid-19 infection
Many of us who were infected in the first wave were unable to access a PCR test to confirm an acute Covid-19 infection unless we were ADMITTED to hospital. I myself attended A&E in the acute stage and had a swab. This was binned as I was sent home the same day. It was policy. I had no evidence I had had an infection. Even the potential symptom list was short. I had countless others. How many of us paid for private antibody tests so we could prove we HAD had it only for those to come back negative too?
Evidence point 1
A diagnosis of a Covid-19 infection can be made by a clinical diagnosis OR through a positive PCR test.
For this we use the WHO classification:
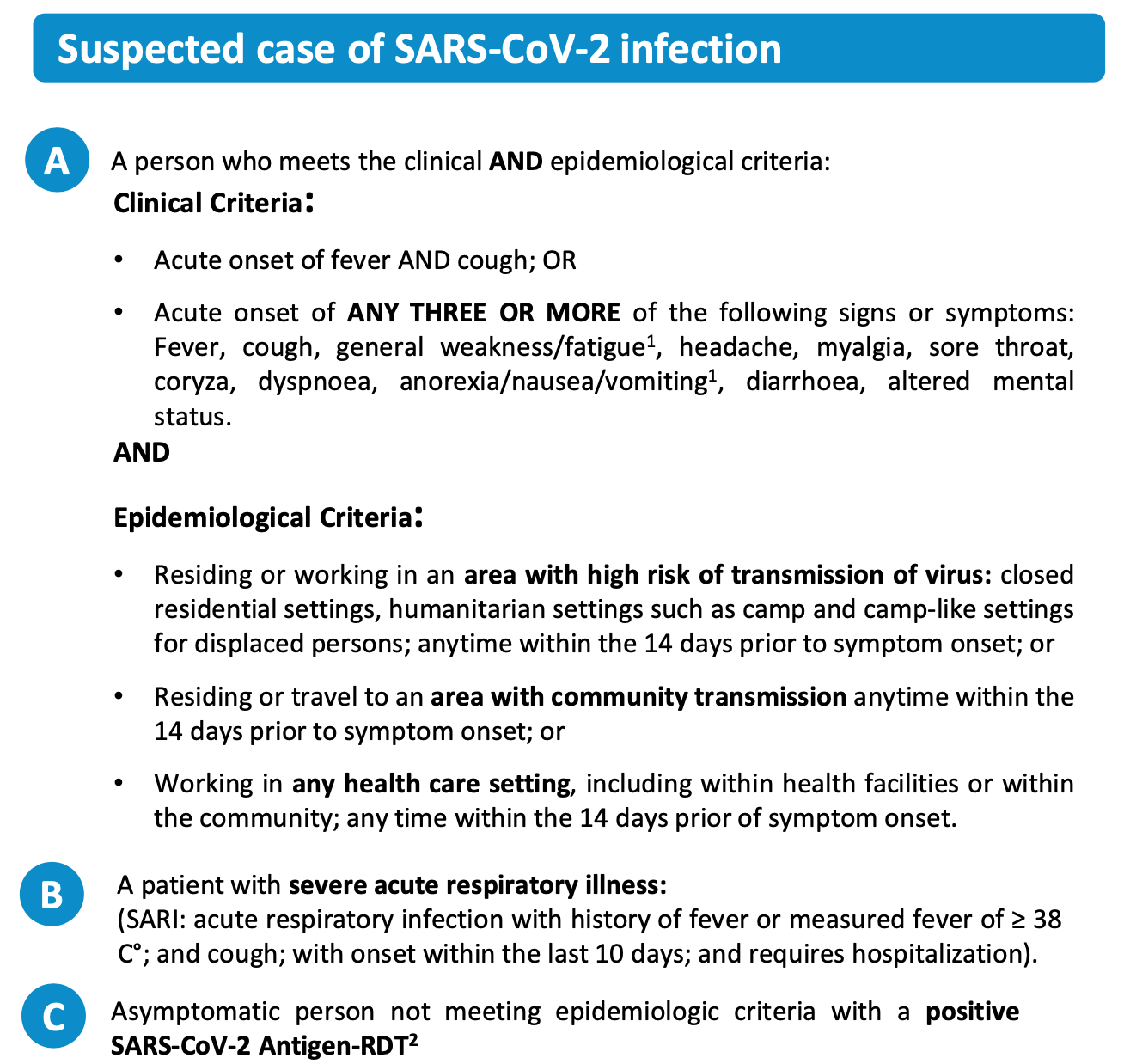
This is useful to know if you didn't fit neatly into the NHSE Covid-19 criteria below:

So an acute Covid-19 infection could be diagnosed with a history of a sore throat with a headache and runny nose (coryza).
Or it could be a stomach-upset like picture - nausea, diarrhoea and fatigue. This just needs to be combined with something like travelling to work where Covid-19 was prevalent.
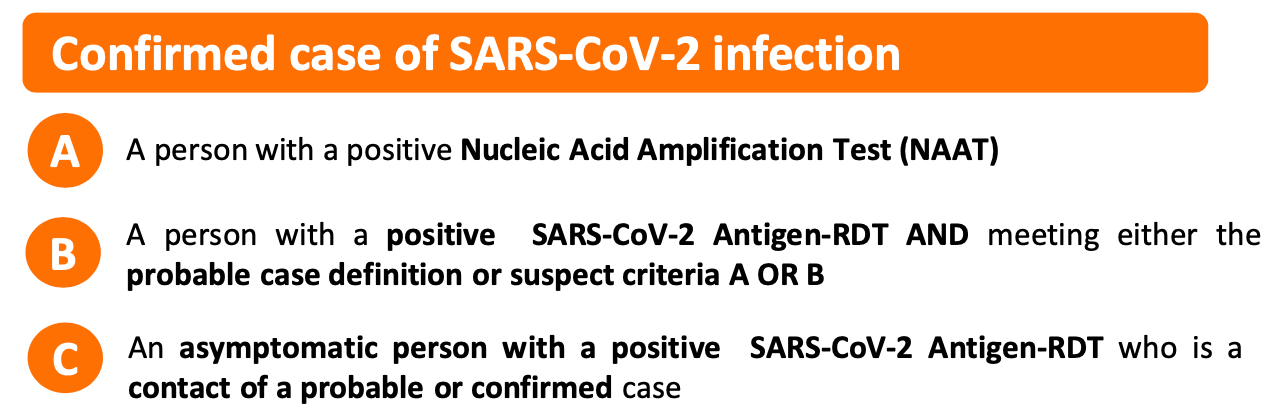
I have included WHO's other definitions for completeness. If you fir the probable or confirmed case there should be no arguments that you have had an acute Covid-19 infection.
The people I am most concerned about is those that had a very mild initial infection (such as a loss of smell that they didn’t notice, or a mild fever, or an upset stomach) or those that were asymptomatic. Both groups won't have even realised they had Covid-19 so would not have gone for PCR testing. As to date I cannot find any data on these groups and how many still went on to suffer LC and if they do how are they going to be able to prove that they ever had Covid-19?
You can however ask your care provider (UK) to use the code LC U07.2 COVID-19, virus not identified
This code can be put into your notes when COVID-19 is diagnosed clinically or epidemiologically but laboratory testing is inconclusive or not available.
Evidence Point 2
An Antibody-negative test result does NOT mean you did not have Covid-19
An antibody test is a blood test that has been used by researchers and hospitals to check if you've had coronavirus (COVID-19) before.
The antibody tests look at the levels/ presence of a specific immunoglobulin/antibody - normally immunoglobulin G (IgG). This is a protective protein produced by the immune system in response to the presence of a foreign substance, called an antigen in our case the SARS-COV-2 virus. They are highly specific to the antigen - this is so if you are exposed to the virus again your body can quickly identify it and destroy it.
For many, many months those of us with negative antibodies were told that we "can't have had Covid-19" which was another blow to getting our validation.
Fortunately with lots of research it has now been found that the test does not work for everyone, as some people who've had the virus do not produce antibodies to the virus.
The UK Government now state that:
Negative antibody test result
A negative result means the test did not detect COVID-19 coronavirus antibodies so it is unlikely you’ve had the coronavirus before.
However, it is possible to have had the virus and receive a negative antibody result. This can happen for some people because they do not develop antibodies, or their level of antibodies is too low for the test to detect.
Long Covid / Post Covid-19 Syndrome
Evidence point 3
ICD-10 is short for the International Classification of Diseases. ICD is the foundation for the identification of health trends and statistics globally, and the international standard for reporting diseases and health conditions. It is the diagnostic classification standard for all clinical and research purposes.It is in its 10th Edition hence ICD-10.
As yet there is no ICD-10 code for Long Covid as it hasn’t been defined. So you really can't be told you can't have something for which there is no definition!
The most current definition of LC/ Post-COVID-19 syndrome used definition has been defined by the National Institute for Clinical Excellence - NICE. It defines LC as:
The signs and symptoms that develop during or following an infection consistent with COVID-19, continue for more than 12 weeks and are not explained by an alternative diagnosis. It usually presents with clusters of symptoms, often overlapping, which can fluctuate and change over time and can affect any system in the body. Post-COVID-19 syndrome may be considered before 12 weeks while the possibility of an alternative underlying disease is also being assessed.
From the recent pre print paper "Recommendations for the Recognition, Diagnosis and Management of Patients with Post Covid-19 Condition - a Delphi Study" it is suggested that care providers should be asked to consider Long Covid in patients with a clinical diagnosis of Covid-19, as per WHO criteria or test-positive, who give a history of new or fluctuating symptoms including but not limited to:
Breathlessness
Chest pain
Palpitations - feeling your heart beating
Inappropriate tachycardia - heart rate persistently raised, or increasing excessively on standing, walking etc
Wheeze
Stridor - a high pitched breath sound
Urticaria - raised itchy rash/ hives
Abdominal pain
Diarrhoea
Arthralgia - painful joints
Neuralgia - stabbing burning pain from a damaged nerve
Dysphonia - voice disorder
Fatigue including neurocognitive fatigue
Cognitive impairment - brain fog, memory issues
Prolonged pyrexia - high temperatures
Neuropathy - weakness, numbness, pain
So I hope in this blog that I have covered the diagnosis of Covid-19 that does not rely upon:
a positive PCR test
a positive antibody test
a narrow range of initial symptoms.
And that the diagnosis of Long Covid is not defined by ICD-10 as yet and can present in many different ways. Your care provider should be considering the diagnosis if you have ANY of the above symptoms and referring you accordingly and in timely manner. The National Health Service for England states the following:
The purpose of this document is to provide commissioning guidance on the development of a specification to assist local healthcare systems to establish post-COVID assessment clinics for patients experiencing long-term health effects following COVID-19 infection. Clinics will offer physical, cognitive and psychological assessments with the aim of providing consistent post-COVID syndrome services for all who need them, whether they were hospitalised or not and regardless of whether clinically diagnosed or by a SARS-CoV2 test.
So even if you have not been diagnosed with Long Covid you can ask to be referred. The more of us that do the more it will become apparent how many of us are still suffering and what services we need.
References
WHO COVID-19 Case Definition https://www.who.int/publications/i/item/WHO-2019-nCoV-Surveillance_Case_Definition-2020.2
UK Government Antibody Testing https://www.gov.uk/government/publications/coronavirus-covid-19-antibody-tests/coronavirus-covid-19-antibody-tests
NICE Long Covid Guidelines https://www.nice.org.uk/guidance/ng188/documents/final-scope
False Negative Tests for SARS-COV-2 https://www.nejm.org/doi/full/10.1056/NEJMp2015897
Rapid Evaluation of Lateral Flow Tests
Waning Antibody Responses in Asymptomatic and Symptomatic SARS-CoV-2 Infection
https://wwwnc.cdc.gov/eid/article/27/1/20-3515_article
Recommendations for the recognition, diagnosis, and management of patients with Post Covid-19 Condition (“long covid”): A Delphi study https://poseidon01.ssrn.com/delivery.php?ID=369003066078011076108087086122067127055013014086045010029076083078091107029080124010106030013042057038011014120121070108070085105016075093037072122120111018031071111038006071094083068108102092100029102095024018093127100112105011107080017065118116125112&EXT=pdf&INDEX=TRUE Not peer reviewed
Antibody testing https://www.biorxiv.org/content/10.1101/2020.11.15.383323v1
National guidance for post-COVID syndrome assessment clinics
DR Kerry Smith Blog - Rose Cottage Doc available here https://www.rosecottagedoc.co.uk/